Many changes during pregnancy affect your cardiovascular system, which includes your heart and blood vessels. Some fluctuations in blood pressure are expected, but hypertensive disorders are still one of the leading causes of maternal and perinatal mortality worldwide.
Hypertensive disorders of pregnancy include chronic hypertension, gestational hypertension, preeclampsia, HELLP, and eclampsia. High blood pressure during pregnancy can place significant stress on your heart and kidneys. This can contribute to heart disease, kidney disease, and stroke. It also increases the risk of preterm birth, placental abruption, and cesarean birth. When blood pressure is too high, it can reduce blood flow to the placenta and limit the oxygen and nutrients available to your baby. This is why your care provider monitors your blood pressure so closely throughout pregnancy.
Most pregnancy-related conditions resolve after birth, but the risk from hypertensive disorders does not end when your baby arrives. Mothers can develop dangerous symptoms in the days and weeks after birth, even if their blood pressure was normal throughout pregnancy. Recognizing warning signs and seeking medical attention right away can be life-saving.
Listen Now
This episode is made possible with support from our sponsors. I appreciate your support for the brands that help power this podcast.
35% off the Zahler Prenatal +DHA on Amazon with code PREPOD35. The Zahler Prenatal +DHA is made with high-quality nutrients like the active form of folate and bioavailable iron. Plus, it includes essential nutrients like omega-3s that you will not find in most other prenatal vitamins. (35% off through 11/30/25. The current promo code is always available here.)

The VTech V-Hush Stroller Rocker is a portable device that gently rocks your baby’s stroller or crib to help them sleep peacefully anywhere. Save 20% with the code VTPODCAST20 and check it out here.

From skin care to treating common pregnancy symptoms like stretch marks, 8 Sheep Organics has you covered. Every product comes with a 100-Day Happiness Guarantee. If you’re not 100% happy with your purchase, simply send them an email and they will get you a refund, no questions asked. Click here to save 10%.
Article and Resources
Hypertension
Hypertension is high blood pressure. The issue with high blood pressure is that the force of blood flowing through your veins is too high. That requires your heart to work harder. According to the American Heart Association, nearly half of American adults have high blood pressure. Usually, there are no obvious symptoms. Over time, this can damage the circulatory system and is a significant contributing factor to heart attack, stroke, and other health threats. Hypertensive disorders affect as many as 10% of all pregnancies worldwide. They are responsible for approximately 10% of all maternal deaths in the United States.
The majority of pregnancy-related conditions disappear after you have your baby. Mothers remain at risk for hypertensive disorders after they have their baby, even if they have no symptoms during pregnancy. Your ability to recognize warning signs and promptly seek medical attention can potentially be life-saving.
Testing Your Blood Pressure
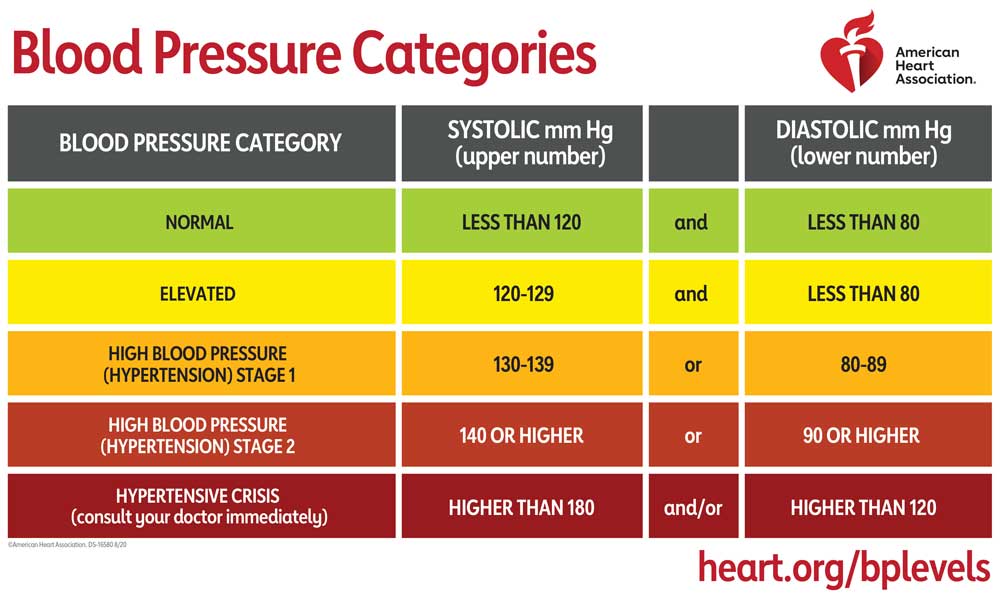
You can expect your care provider to test your blood pressure with a blood pressure cuff at each prenatal appointment. This goes around your arm, and they pump it up with air to cut off the blood flow. The air is slowly released, and your blood starts flowing again. Two measurements are taken of your blood flow, measured in millimeters of mercury (mm Hg). The systolic reading is how much pressure your blood is exerting against your artery walls when the heart beats. The diastolic reading is how much pressure your blood is exerting against your artery walls while the heart rests between beats. These two numbers are combined to give you a number like 120/80 mm Hg (systolic/diastolic). Ideally, your blood pressure is below 140/90 mm Hg.
How Your Cardiovascular System Changes in Pregnancy
Many changes during pregnancy affect your cardiovascular system, which includes your heart and blood vessels. Some cardiovascular changes can be noticeable as spider veins or varicose veins. Spider veins are tiny red or bluish veins that most often appear on your legs. Other than changing the appearance of your skin when they are visible, they are painless. Varicose veins are more prominent, protruding veins. Varicose veins have the potential to be uncomfortable for some women who experience them. See this episode for more information on the prevention and treatment of spider and varicose veins.
During pregnancy, you increase your blood volume by up to 45%. As a result, your heart has to work harder to circulate that extra blood. Your heart rate increases during pregnancy by 10 to 20 beats per minute, a 20% to 25% increase. Hormonal changes dilate and relax your veins. This causes your blood pressure to decrease early in your pregnancy through the second trimester. Then increase in the third trimester and postpartum.
Hypertensive Disorders of Pregnancy
While some changes in blood pressure are normal and expected during pregnancy, hypertensive disorders are one of the leading causes of maternal and perinatal mortality worldwide. Hypertensive disorders of pregnancy include chronic hypertension, gestational hypertension, preeclampsia, preeclampsia with severe features, HELLP (hemolysis, elevated liver enzymes, and low platelet count), and eclampsia. High blood pressure during pregnancy can put extra stress on your heart and kidneys, which can lead to heart disease, kidney disease, and stroke. As well as increasing your risk for preeclampsia, preterm birth, placental abruption, and cesarean birth. High blood pressure can also reduce blood flow to the placenta, affecting the flow of oxygen and nutrients to your baby. You can see why your care provider closely monitors your blood pressure throughout your pregnancy.
Chronic Hypertension
Chronic hypertension is high blood pressure before pregnancy or that develops within the first 20 weeks of pregnancy. Since blood pressure decreases in the first half of your pregnancy, expectant mothers with mild hypertension may see their blood pressure temporarily return to normal levels.
Gestational Hypertension
Gestational hypertension occurs when you have normal blood pressure before you are pregnant, and in the second half of your pregnancy, your systolic blood pressure is above 140 mm Hg, or your diastolic blood pressure is above 90 mm Hg.
Preeclampsia
Preeclampsia is a more serious pregnancy disorder. This is associated with new-onset hypertension, which occurs most often after 20 weeks of gestation and frequently near term. This is estimated to affect between 2-8% of pregnancies. In the United States, the rate of preeclampsia increased by 25% between 1987 and 2004.
How Preeclampsia is Diagnosed
The main criteria for diagnosing preeclampsia are high blood pressure and high levels of protein in your urine. ACOG defines this as Systolic blood pressure of 140 mm Hg or more or diastolic blood pressure of 90 mm Hg or more on two occasions at least 4 hours apart after 20 weeks of gestation in a woman with previously normal blood pressure. If you have high blood pressure but not high protein in your urine, other factors may be considered. These include results from a blood test showing a low blood platelet count or issues with your liver or kidneys, fluid in your lungs, or headaches.
Symptoms of Preeclampsia
While you may not detect that your blood pressure is high or whether there is protein in your urine, there are common symptoms you may notice. The symptoms of preeclampsia include swelling in your face or hands, persistent headache, changes in your vision or seeing spots, pain in your upper abdomen or shoulder, nausea and vomiting in the second half of your pregnancy, sudden weight gain, and difficulty breathing.
Preeclampsia Risk Factors
There are many factors that can increase your risk for preeclampsia. This condition is more common in first-time mothers, mothers who had preeclampsia in a previous pregnancy, or those with twin or multiple pregnancies. If you have hypertension, diabetes, or gestational diabetes, you are at a higher risk. Blood clotting disorders like thrombophilia or antiphospholipid antibody syndrome, kidney disease, and systemic lupus erythematosus, the most common type of lupus, increase the risk. Additionally, maternal age over 35, using assisted reproductive technology, obstructive sleep apnea, and a prepregnancy BMI over 30 also put you at a higher risk of preeclampsia.
Screening Tests for Preeclampsia
There are some tests to screen expecting mothers for preeclampsia. A screening test only gives you the likelihood of a condition. It cannot give a diagnosis. Unfortunately, none of the screening tests for preeclampsia are very accurate, especially in low-risk women. The positive predictive value of these tests ranges from 8% to 33%, meaning the tests only identify 8-33% of patients who will develop preeclampsia, missing most of the mothers who will develop this condition. ACOG’s position is that biomarkers and ultrasonography cannot accurately predict preeclampsia and should remain investigational.
Preeclampsia with Severe Features
Gestational hypertension is considered severe when the systolic level reaches 160 mm Hg, or the diastolic level reaches 110 mm Hg, or both. If your blood pressure exceeds these values, you may be diagnosed with preeclampsia with severe features.
HELLP (hemolysis, elevated liver enzymes, and low platelet count) Syndrome
HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome is a dangerous complication of preeclampsia. The main symptoms of HELLP syndrome are right upper quadrant pain and generalized malaise in up to 90% of cases, and nausea and vomiting in 50% of cases.
Eclampsia
Eclampsia is even more severe and includes seizures. Although eclampsia is serious, it only affects 0.3% of pregnancies in the United States, which is significantly lower than in many developing countries. ACOG notes that it is important to understand that there is not a linear progression from preeclampsia to preeclampsia with severe features to eclampsia. Seizures occur in a small number of cases of preeclampsia, 1.9%, and in 3.2% of cases of preeclampsia with severe features. 20–38% of cases of eclampsia occur without the classic signs of preeclampsia before the seizure episode.
Hypertension and Prenatal Care
Your doctor or midwife will take your blood pressure at each prenatal appointment. If your provider diagnoses you with any type of gestational hypertension, you can expect additional monitoring throughout your pregnancy. You may have prenatal appointments more often. Your care provider may also ask you to monitor your blood pressure at home and do a daily kick count. Your doctor could recommend additional ultrasounds to monitor your baby’s growth or other tests like a biophysical profile or non-stress test, later in the third trimester.
The level of additional monitoring depends on your symptoms and diagnosis. Gestational hypertension or preeclampsia without severe features may be treated in a hospital or as an outpatient with frequent visits to your doctor. Preeclampsia with severe features may be treated in the hospital.
Low-Dose Aspirin
There is quite a bit of evidence that low-dose aspirin may reduce the risk of preeclampsia in some women. Low-dose aspirin comes in 81 mg tablets, compared to a standard tablet containing 325mg. ACOG recommends low-dose aspirin if you are at high risk of developing preeclampsia or you have two or more moderate risk factors for preeclampsia.
You are at a high risk of developing preeclampsia if you have a history of the condition or hypertension, if you are pregnant with twins or multiples, have gestational diabetes, renal disease, or an autoimmune disease. Moderate risk factors include a BMI over 30, a family history of preeclampsia, sociodemographic characteristics if you are Black or low income, are over 35, and if you had a previous pregnancy with a low birth weight or small for gestational age baby, and if there have been more than 10 years since a previous pregnancy.
The optimal time to start taking low-dose aspirin, if your doctor prescribes it is after 12 weeks and ideally before 16 weeks. Like any medication, even if it is available over-the-counter, talk to your care provider before taking it.
Inducing Labor Early
For low-risk women without hypertensive disorders, ACOG supports elective induction at 39 weeks. If you have gestational hypertension or preeclampsia without severe features, your doctor may recommend induction at 37 weeks. This recommendation is based on a randomized controlled trial that found that inducing labor before 37 weeks in women with gestational hypertension or preeclampsia without severe features improved maternal outcomes.
If you have preeclampsia with severe features, you and your baby are at a higher risk of complications. If you are less than 34 weeks, your doctor will closely monitor you. As long as your condition is stable, they will likely recommend inducing labor at 34 weeks. Even before 34 weeks, if the health of you or your baby worsens, your doctor may recommend immediate delivery.
Any decision to induce labor early involves weighing the risks and benefits and taking into account the particulars of your condition. See this episode for a deep dive into inducing labor, including the evidence, how it works, and the risks and benefits of every different method of labor induction.
Interventions During Labor and Birth
If you have a hypertensive disorder, your doctor may recommend magnesium sulfate during labor to prevent seizures. In women with preeclampsia, evidence shows magnesium sulfate more than halves the risk of eclampsia and reduces the risk of placental abruption. The most commonly reported side effect was hot flushes, and this intervention increased cesarean births by 5%.
While vaginal birth is preferred, mothers with hypertensive disorders are at a higher risk for cesarean birth. One analysis found the probability of cesarean delivery in women with hypertensive disorders was 39.5% versus 26.8% in those without the diagnosis. When adjusted for other risk factors, including obesity, diabetes, and induction of labor, the probability was 35.1% in the hypertensive group compared to 26.4%. ACOG states that with labor induction in preeclampsia with severe features, the likelihood of cesarean delivery at less than 28 weeks of gestation could be as high as 97%, and at 28–32 weeks of gestation as high as 65%.
You and your doctor need to consider many factors in the decision to perform cesarean delivery. If you have any hypertensive disorder, you should be knowledgeable about cesarean birth. You have many options for cesarean, but you need to know what those options are. Educating yourself about cesareans can make a massive difference in feeling prepared and confident going into the procedure. There are episodes of the Pregnancy Podcast on cesarean birth and gentle cesarean and vaginal seeding that can prepare you for what to expect and explain your options.
Postpartum Preeclampsia
The majority of pregnancy-related conditions disappear after you have your baby. Unfortunately, mothers remain at risk for hypertensive disorders after birth, even if there were no symptoms during pregnancy. ACOG states, “It is important to increase the awareness among health care providers and to empower patients to seek medical advice if symptoms that precede eclampsia, hypertensive encephalopathy, pulmonary edema, or stroke are noted in the postpartum period. Most women who present with eclampsia and stroke in the postpartum period have these symptoms for hours or days before presentation”.
A review in the American Journal of Obstetrics and Gynecology outlines the need for more research on postpartum preeclampsia. The journal notes that approximately 60% of patients with new, delayed-onset postpartum preeclampsia have no antecedent diagnosis of a hypertensive disorder of pregnancy. Most women with delayed-onset postpartum preeclampsia present within the first 7 to 10 days after delivery; however, this varies widely in the literature, with an onset of up to 3 months after delivery reported. Women most frequently present with neurologic symptoms, typically headache, which has consistently been reported as the most common symptom in approximately 60% to 70% of women across multiple studies.
Warning Signs
Your ability to recognize warning signs and promptly seek medical attention can save your life. The days and weeks after you have your baby can be a blur with birth recovery, sleep deprivation, breastfeeding, and caring for a newborn. The Preeclampsia Foundation outlines warning signs to watch out for, when to call your doctor, and when to go to the ER or call 911.
Call your healthcare provider right away if you experience:
- Blood pressure at or exceeding 140/90
- Severe headache that will not go away
- Vision changes
- Stomach pain
- Swelling in your hands or face
- Feeling nauseous or throwing up
Have someone take you to the Emergency Room or call 911 if you experience:
- Blood pressure at or exceeding 160/110
- Shortness of breath or trouble breathing
- Seeing spots
- Seizures
The only way to know your blood pressure is to measure it with a blood pressure cuff. It is not universally recommended that you purchase one for home use after having your baby. If you already own one, you may ask your doctor or midwife about monitoring your blood pressure postpartum.
Contacting Your Doctor or Midwife
Postpartum prenatal appointments are an excellent opportunity for your doctor to check your blood pressure or discuss your birth recovery. Unfortunately, you may go weeks from the time you have your baby until you see your doctor or midwife. ACOG’s guidelines call for a visit within three weeks of birth, which is well outside the 7-10 day window that postpartum preeclampsia usually shows up. If you had any hypertensive disorder during pregnancy, you may have an appointment sooner.
Reach out to your doctor or midwife right away if you have any symptoms or concerns. If it is outside business hours or you cannot reach them, you can always go to the labor and delivery unit or the ER. Trust your gut, and if something doesn’t feel right, do not delay seeking medical care.
Advocating for Yourself
It can be challenging to advocate for yourself in the event you do not feel like your care provider is addressing your symptoms or concerns. If you visit your doctor or the emergency room, having your partner or someone with you to help you advocate can be helpful. If you visit the ER, be sure to tell them you recently had a baby, and you may request to see an obstetrician.
Knowledge is Power
While hypertensive disorders are serious, your care provider will monitor you and your baby closely. There are medications and interventions designed to keep you and your baby healthy. Navigating pregnancy with high blood pressure can be challenging. Hopefully, this article has given you a good base of information. Even if you are unaffected by high blood pressure during your pregnancy, there are important warning signs you should be aware of after you have your baby. The goal of this article is not to scare you but to educate you. Identifying warning signs and seeking immediate medical treatment could potentially be life-saving.
Thank you to the brands that help power this podcast.
Save 35% off the Zahler Prenatal +DHA on Amazon with the code PREPOD35.
Zahler goes above and beyond using the latest scientific research to formulate their Prenatal +DHA with high-quality nutrients like the active form of folate and bioavailable iron. Plus, it includes essential nutrients like omega-3s that you will not find in most other prenatal vitamins. Not all prenatal vitamins are created equal. This vitamin is carefully formulated with the nutrients you and your baby require in the optimal ratios for absorption, metabolism, and safety. (35% off through 11/30/25. The current promo code is always available here.)
Save 20% OFF the VTech V-Hush Stroller Rocker with Code VTPODCAST20
The VTech V-Hush Stroller Rocker is a portable device that gently rocks your baby’s stroller or crib to help them sleep peacefully anywhere. With three adjustable motion levels, you can choose the perfect calming rhythm for your baby. It also includes a built-in amber night light, a rechargeable battery, soothing sounds, white noise, and lullabies. Soothe your baby to sleep anywhere with the V-Hush Stroller Rocker. Save 20% with the code VTPODCAST20 and check it out here.
8 Sheep Organics makes amazing, 100% clean, natural pregnancy products. From skin care to treating common pregnancy symptoms like insomnia and stretch marks, 8 Sheep Organics has you covered. Every product comes with a 100-Day Happiness Guarantee. You can try it completely risk-free for 100 days. If you feel the product has not worked for you, or if you’re not 100% happy with your purchase, simply send them an email and they will get you a refund, no questions asked. Click here to save 10%.